Guiding principles for Telehealth design
Why placing patients at the centre of Telehealth design is an obligation, not just about simply following UX best practices.

It’s Healthtech time
Imagine you are not feeling well. Nothing serious, you don’t need to call an ambulance, but you probably want to go see your family doctor. You are going to call the clinic and set an appointment. If you are lucky, there will be an opening for you within a few days, for others, within a couple of weeks, and for many unlucky people, there isn’t even an option because they don’t have a family doctor. You are writing down the time and day of your appointment on a sticky note to enter the appointment later on your smartphone’s calendar. In spite of receiving calendar invites via email all day long for most meetings you have, for this one there will be no email follow up. The earliest available time is inconvenient because it falls right in the middle of your workday. You consider the travel time and realise you may need to skip lunch that day. You agree to this time anyway because you need to see your doctor and this is the earliest availability.
On a good day, many of us have become used to managing the above scenario. However now, during the Covid-19 pandemic, leaving your house and attending a non-emergency doctor visit is likely not an option. Luckily, the future of a family doctor office visit is changing. It is changing using smartphones, video conferencing, chats, and all things digital. The change has been slow in the making but the current pandemic is helping to speed up the process. Many healthcare systems around the world together with government agencies and startup companies are building and delivering Telehealth solutions — the future of non-emergency and routine healthcare delivery.

Telehealth is the umbrella term for digitising the interaction between patients and the healthcare system. This is not limited to visits to your family doctor. It covers the interaction between patients and many other types of healthcare professionals including nurses, specialists, and mental health practitioners. In March 2020 the Centers for Medicare & Medicaid Services in the United States announced that under the pandemic emergencies act an expanded list of practitioners will now be able to provide Telehealth services, such as all doctors, nurses, clinical psychologists, and licensed clinical social workers. It is safe to assume that a lot of these accelerated measures are likely to stick around in the post-pandemic world.
The United States continues to lead advancements in Telehealth (also known as Telemedicine) following Vice President Al Gore specifying telemedicine as a key component of the National Information Infrastructure back in 1992. The concept slowly evolved for over 30 years prior to that. Canada, although slightly behind the USA, has seen a rise in the use of technology in healthcare delivery in the past decade. Technology use is accelerating in Canada, mainly through regional NGOs such as the Ontario Telemedicine Network. As well, additional funding just announced by the government in response to the pandemic will see a focus on the inclusion of mental health services in Canadian Telehealth. European countries also lag behind the USA as suggested by Research 2 Guidance, however, now Germany is leading a similar acceleration movement in Europe with its ‘Fast Track’ program. The North American and Western European markets outlined above bring together two important challenges: strict security and privacy regulations, and scale. Advancements in digital healthcare are not limited to these markets and can be seen all around the world. Israel for example, with much looser privacy concerns, has been practising Telehealth for quite some time and could be a good place to look for healthtech product innovation examples. Even before Telehealth solutions were launched elsewhere in the world, Israel had digitalised medical records decades earlier. Today, many other countries are still struggling with their healthcare digital transformation.
Navigating Healthtech challenges
The above snapshot of healthtech in different markets demonstrates the increase in Telehealth related solutions that we will need to design and develop for in the immediate future. It’s true that the specific issues of the Covid-19 pandemic, such as social distancing, helped accelerate some of the Telehealth efforts. However, the needs for Telehealth are far-reaching and will likely define the future of healthcare delivery regardless of the current situation. If you work in design and tech but have never worked with the healthtech industry you probably wonder why changes are taking so long. In my career, I’ve worked with slow-changing industries such as fintech, education, and healthtech. In fintech one of the greatest challenges is to overcome complex legacy technology. In public education, convoluted, bureaucratic administration and unionised workforces present challenges to the adoption of new technologies. In healthtech though, it appears there are few legacy technologies to overcome or even any existing technology to replace at all. Nor are bureaucracies or unionised workforces a major inhibitor. Many innovative solutions for Healthtech, such as Telehealth, don’t seem to impose any challenges that haven’t already been solved in other domains. For example, facilitating digital communication, securely sharing documentation and information, and tracking and making sense visually of data. Taking a user-centred design approach easily uncovers simple solutions for most use cases in Telehealth. So what is it in the Telehealth space that makes it so difficult to bring solutions to market quickly if design and technology are not the issues?
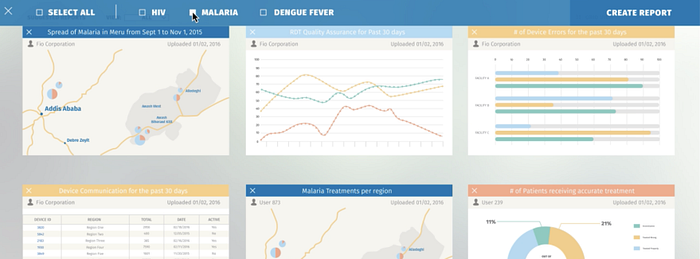
In 2016 I led an interdisciplinary design team, during a think-tank exercise, to develop foresight strategies for a healthcare system which capitalised on big-data and emerging technologies. One of the challenges was to model a system that increases the efficiency of healthcare delivery while depending on existing resources. Telehealth quickly emerged as an essential component in making this model happen. Conceptually, thinking of solutions is not too difficult. However, I found that bringing solutions to life is like running in a track and field race with many barriers to jump over. While working on a data analysis system that tracked the spread of infectious diseases I was exposed to many compliance challenges — privacy being an obvious, major concern. Tracking the spread of HIV in Kenya was an easier task due to less strict privacy regulations than in the US for example. Designing a global system to scale across different regulatory jurisdictions means that design teams need to be aware of and account for all of the different compliance requirements in existence. Differences are not only limited to complex regulations such as privacy and security but also concerning governmental administrative processes.
One example of complex administrative processes is billing for healthcare services. Automated billing for most industry sectors is a complicated problem to solve. Healthcare adds a layer of complexity given that most of the systems in which medical professionals bill for their services are highly convoluted. If you’ve ever thought that tracking time as a creative freelancer is time-consuming, consider doctors who must track every task for every interaction separately and are often required to bill a different rate for each task. I dealt with this design challenge when consulting on the design of a specialised billing tool for medical specialists in Ontario. The government assigns billing codes to certain tasks and procedures and the tracking and reporting on those can become so complicated and time-consuming that many doctors hire accounting firms to manage billing on their behalf. This doesn’t completely eliminate a doctor’s responsibility for tracking day-to-day activity or reporting activity to the doctor’s accounting team, or admin team in a clinic setting. When patients’ information is either missing or inaccurate in the billing report, doctors in Ontario end up losing revenue. On the other hand, when billing code errors are made, the system loses money by overpaying for unperformed procedures. In a public healthcare system, like the Canadian one, Provincial governments are bearing those costs. But this is not limited to Canada; it is also prevalent in other systems such as in the US where some institutions suggest over 80% of medical bills contain errors. In this privatised system, insurance companies and individuals end up bearing the costs of the mistakes.
If medical billing wasn’t already very complicated to begin with, integrating Telehealth into it just makes it even more complex.
In early April 2020, the American Centres for Medicare & Medicaid Services hosted an open forum on Telehealth changes during Covid-19. The Q&A session was very quickly dominated by questions borne from confusion about billing codes for Telehealth services. The expansion of Telehealth to include a wider spectrum of medical services seems to cause integration issues. Again, this is not a localised problem. Recently in Ontario, Canada the Provincial health ministry acknowledged having problems processing payment for Telehealth services. It can be assumed that as long as doctors are able to communicate with their patients, Telehealth services can be delivered. The lack of sophisticated systems and great user interfaces don’t seem to be the main barrier to delivering services; many doctors simply resort to phone calls. A major caveat seems to be the integration of ever-changing administrative processes into a digital ecosystem.
In order to address the list of Telehealth design challenges, it’s beneficial to form interdisciplinary design teams covering service design, strategy, research, and user experience together with IT. Systems will be meaningful if they address the needs of all user types including patients, medical professionals, and administrators. Such systems will need to integrate with other services, databases, and government portals. On the technical side, such scenarios increase the likelihood of both user and integration errors, which could hinder usability.
Interdisciplinary design teams should develop a confident level of subject matter expertise in order to predict and account for a unique list of error handling requirements for administrative healthtech products.
With respect to compliance, any product company that aims to operate in the US should be familiar with the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and its privacy, security, and information technology requirements. A good place to get digestible information about HIPAA requirements for business is through the Department of Health & Human Services.
Guiding Principles for Telehealth Design
Today’s Telehealth environment consists of a global ecosystem of myriad digital solutions often developed and designed separately. The two main areas of Telehealth services according to the World Health Organization are:
- Telecare: also known as remote assistance and teleconsultation. This service is concerned with follow-ups, diagnosis, and treatment.
- Telemonitoring: which is usually concerned with chronic-patients, and often includes the recording of biological parameters.
Telehealth services have seen massive growth in the past decade; even prior to the Covid-19 related increase in demand. Given this growth, it is likely that many of us will find ourselves soon working directly or indirectly in the Telehealth space if we haven’t done so already.
Establishing fundamental principles to guide Telehealth design will help us keep sight of the user experience and user journey throughout different healthcare systems.

Although this may sound like common sense to many of you — it seems to be easier to say than it is to do. In 2015 the U.S. Department of Health & Human Services published a whitepaper Designing The Consumer-Centered Telehealth & eVisit Experience. The paper says a lot, including introducing a list of nine “Consumer-Centered Telehealth Design Principles”. The list, however, consists of only basic principles of user experience design and does not provide anything more concrete to specifically define a healthcare experience (i.e. steps on what to do). Some of the principles offered include: “#1 There cannot be friction for the user”; “#4 We must be sensitive to data overload”; “#8 Integrate technology & human interaction in the physical world.” and so on. While the paper cites 41 educated and accomplished professionals who attended workshops and contributed to its findings, it seems that none of these professionals has obvious experience in user experience design. Furthermore, there is no mention of including user input and consumer perspective in this fundamental piece of work, which in my opinion leaves more questions than answers.
Conversely, the World Medical Association (WMA) published its own statement on Guiding Principles for the Use of Telehealth for the Provision of Health Care. The list of 6 principles included appears infinitely more specific for the Telehealth use case than that published by the U.S. Department of Health. The principles by the WMA represent the clinical and healthcare delivery point of view and don’t necessarily provide an end consumer/patient point of view. This sheds light on a critical problem we need to address in our work. In the design of solutions that facilitate interaction between healthcare providers and patients, there are two different end-user perspectives. Most of the institutional work done so far seems to be focused on healthcare providers’ end-user type. Neglecting the point of view of the patients’ end-user type can easily create experience problems in a brand new system.
An opportunity exists today to support the patient experience by reimagining the healthcare system from a patient-first perspective
During the Healthcare & Big Data design exercises I led in 2016 (mentioned earlier), a patient-centric user journey led to the following guiding principles:
- Availability: availability of care to everyone, telemedicine access to a range of specialised medical professionals and their aggregated assessment knowledge, easy access to testing.
- Efficiency: fast access to healthcare services, reduce waiting times to the bare minimum, digitalisation of all non-emergency first diagnosis procedures.
- Prevention: access to health education, empowering patients to continuously self-test, monitor, and aggregate self-health data.
- A new strategy for Data Management: including patients’ collection and control, and exchange of aggregated data with monetary resources from interest groups.
This system was based on a paradigm shift which put the patient in the focal point. The hypothesis is that a patient-centric design will make a ‘better patient’ which will make a better healthcare system. A better patient means a patient who is more knowledgeable and health-conscious, empowered and incentivised to take preventative actions and is in control of their health data.
Placing patients in the centre of the system will drive the development of tools and means to empower patients to become healthier. Healthier populations reduce the overall costs and burden on the healthcare system. This leaves the limited resources of care for emergencies and treating chronic conditions requiring specialised care the most.
Prevention seems to be a key differentiator when comparing the clinical centric approach to Telehealth design principles vs a patient-focused one.
From the above conversation we can derive that there are two alarming end-users trends we should pay attention to when considering Telehealth design and solutions:
- what doctors struggle the most with, and
- what patients do in the absence of the tools they need.
Doctors burnout is a serious issue. One major reason for physicians burnout is due to their “struggle to keep up with a soaring burden of administrative tasks.” This issue has serious implications that should not be taken lightly. On the other end of the Telehealth spectrum, there are patients. Patients who are active users managing their own health will resort to potentially harmful alternatives when the system doesn’t provide them with the right solutions.
Dr Google is always there when healthcare systems are not
Compounding the issues relating to seeing a family doctor for those with the option to do so, is the fact that millions of Canadians still don’t have access to family doctors. In fact, Canada ranks very low in the number of practising physicians per population in comparison to its OECD counterparts. Seeing a doctor is also very expensive for those who do not have the privilege of access to public healthcare. The costs of healthcare in the US are very high, and we hear about it often, but healthcare cost is a global problem that pushes millions into poverty. Continuous care, normally supported by a family doctor, is very important and the lack of it negatively affects healthcare systems worldwide. Telehealth can help address many of these issues by improving access, availability, and efficiency. Meanwhile though, in the absence of easy access to doctors, people find alternative routes to answers, because when you feel bad you can’t move on until you get clarity.
Online self-diagnosis tools (e.g. WebMD) are very popular with end-users because of the high availability (accessible from any internet-enabled device) and perceived efficiency. Often those online symptoms checkers are wrong. But this is not preventing people from seeking medical advice from Dr Google “which, for many adults, has become a de facto primary care doctor.” This is an alarming trend.
It is therefore imperative that Healthtech solutions, such as Telehealth, be designed around patients to arrest the shift to self-diagnosis via online health checkers that exclude healthcare practitioners from the patient journey. Examining the issue from a user perspective shows us that regardless of the inaccuracy and potentially harmful advice users obtain online, the human urge to take action is very powerful. The urge to self diagnose, seeking prompt answers and address the unknown takes precedence over common sense and logical thinking.
Recognising the impact on human well-being resulting from the lack of availability, access, and patient-first experience; placing the patient at the centre of Telehealth design is not simply following UX best practices but an obligation.